The United Nations has set a goal of ending the global HIV/AIDS epidemic by 2030.
The tide is slowly turning in southeastern Africa — which encompasses countries like South Africa, Mozambique, Lesotho and Botswana — and which remains the epicenter of the epidemic and home to more than half the 36.9 million people living with the disease. The rates of deaths and infections there are declining overall. But a July 2018 report from the United Nations’ AIDS agency found a $5.4 billion shortfall in global funding needed to achieve final victory.
A first-of-its-kind new map may help increase the precision of the HIV/AIDS response as some data-savvy researchers narrow their focus on the continent’s worst-affected areas — to the size of a small town.
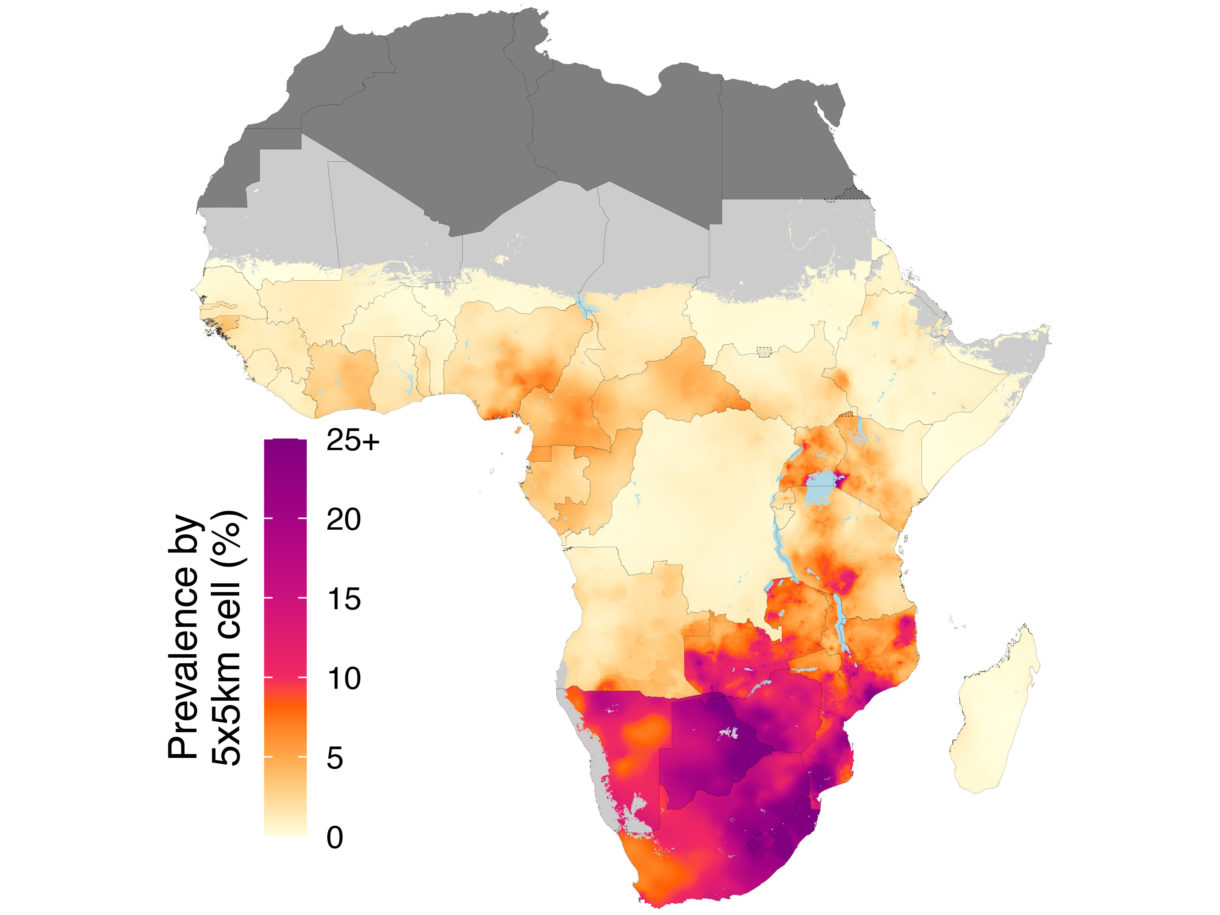
A study published Wednesday presents what these researchers describe as the most detailed map ever produced of HIV prevalence across sub-Saharan Africa. The team behind the map is an international consortium of epidemiologists led by the University of Washington-Seattle’s Institute for Health Metrics and Evaluation. Their work appears in the peer-reviewed journal Nature.
The researchers don’t just go country by country. They break down the continent into a grid of thousands of 9.6-square-mile squares. The result is a view of HIV distribution that is much more fine grain than the usual national- or province-level data and that could have a huge impact on how resources are allocated to diagnose, treat and prevent new infections.
Researchers have long understood that local economic, cultural and political conditions — including rates of male circumcision, drug use and attitudes toward homosexuality and sex work, not to mention funding for prevention and treatment programs — can determine who is vulnerable to HIV infection and how people living with the disease access treatment. That leads to pockets of infection that prove stubbornly resistant to progress.
The epidemic is very unevenly spread, the study found. Of the roughly 25 million HIV-positive people in sub-Saharan Africa, a third live in very small, highly concentrated pockets: the 0.2 percent of grid squares that have more than 1,000 HIV-positive people living in them. The remaining two-thirds are spread out more broadly. In a majority of the continent, the epidemic is almost nonexistent.
“There’s an increasing appreciation that this epidemic is even less homogeneous than people have imagined,” says Wafaa El-Sadr, global director of the public health organization ICAP and a professor at Columbia University, who was not a contributor to the study (one of her ICAP colleagues, Jessica E. Justman, was a co-author). “This kind of data helps to prompt other research questions: Can we do different kinds of interventions in these places?”
Chido Dziva Chikwari, a Zimbabwean-based infectious disease researcher with the London School of Hygiene & Tropical Medicine, says Zimbabwe’s Matabeleland South province is the kind of localized HIV hot spot that can be crucial in developing new strategies for fighting the epidemic. Chikwari, who was not involved in the study, and her colleagues have been working to understand why the province, home to around 700,000 people in an area the size of West Virginia, has the country’s highest rate of HIV prevalence — 22.3 percent of the population is infected, compared with the national average of 14.6 percent.
A key driver, they’ve found, is economic migration: The province shares a border with an area in Botswana where the rate of HIV prevalence is at least 25 percent. Zimbabweans from the province, especially men, frequently travel there for work — and often pick up new sexual partners on the way.
“It’s a migrant population,” she says, “and that changes the sexual networks.”
In addition to creating new pathways for infection to spread, the population’s mobility also makes infections harder to treat. Antiretroviral medication, the standard treatment for HIV, must be taken daily, and workers in Matabeleland South were missing doses because their frequent travel made it difficult to pick up their prescriptions. So two years ago, Zimbabwe introduced a new policy that allows members of HIV-positive peer support groups to pick up and distribute each other’s medications. Chikwari believes that this simple innovation could have a big impact on access and adherence to treatment.
“We’ve done sweeping interventions, and they work to an extent,” she says. “But we’re now reaching the last mile, so we need innovative ways to target the last vulnerable populations.”
To identify these holdouts, the researchers from the Institute for Health Metrics and Evaluation analyzed a mountain of existing HIV data from 2000 to 2017. They compiled 134 public health surveys conducted by a mix of governments, academic institutions, companies and nongovernmental organizations in 41 African countries, as well as data from nearly 2,000 prenatal care clinics across the continent that routinely test pregnant women for HIV. They paired each data point with a GPS location tag and fed it into a statistical model that produced estimates for every grid square and was able to calculate where and by how much HIV prevalence has changed over the last two decades. The study grew out of a $279 million grant to IHME from the Bill & Melinda Gates Foundation in 2017 to support research on “critical data about global health trends.” (The foundation is a funder of NPR and this blog.)
The study opens an entry point for further research on why prevalence is rising in some areas and decreasing in others, says lead author Laura Dwyer-Lindgren, an assistant professor of health metric sciences at IHME. But it’s not just valuable for long-term programs. In the short term, it provides a snapshot of where the need for treatment and prevention resources is highest.
“The story is changing,” she says. “You can see how the number of people who are in need of treatment, and where those people are concentrated, is shifting over time.”
The study doesn’t reveal all facets of the epidemic. Its data cover only people ages 15 to 49 and don’t account for differences in prevalence within that age group or for children. And prevalence, as a metric, has limitations. It doesn’t reveal much about how quickly the epidemic is or isn’t spreading. A rising prevalence rate might be a good thing if it indicates that people are living longer after being infected.
But prevalence is a good indication of how many people are in need of treatment, El-Sadr says. And combined with other information on local treatment and prevention programs, demographics and the rate of new infections, prevalence can yield invaluable insights about which solutions work and which don’t.
In a world with constrained public health resources, precision maps are also essential to directing spending on facilities, workers and medicine, says Matthew Kavanagh, director of the Global Health Policy & Governance Initiative at Georgetown University, who was not involved in the study. Low-concentration areas are especially expensive to confront, he says, since they still contain the majority of HIV-positive people but can’t implement testing and treatment efficiently.
But identifying the small number of highest-concentration areas could help target saturation-level treatment and prevention efforts, he says. Take the goal of providing access to prophylactic treatment for every single person in the community, which has traditionally seemed cost prohibitive. Previous research has shown that because some HIV hot spots — cities, for example — tend to be the source of infections for a wider area, intensive HIV treatment in those places could ripple out to reduce transmission rates across the region.
“We still have not gotten to the point where we’re really reaching everybody in those hot spots,” he says. “This data paints a really useful, if complicated, picture for what we need to do to address HIV.”
Tim McDonnell is a journalist covering the environment, conflict and related issues in sub-Saharan Africa. Follow him on Twitter and Instagram.
9(MDEwNzczMDA2MDEzNTg3ODA1MTAzZjYxNg004))